
Welcome to another section of the MacIver 2021-2023 State Budget Analysis series. Here we’ll go through the budget for the Department of Health Services (DHS) and talk about public health proposals by the Governor that were removed by the Joint Finance Committee (JFC).
The most contentious, and perhaps the most expensive, item that JFC removed from the budget before passage was the expansion of Wisconsin’s Medicaid program, BadgerCare. Governor Evers proposed expanding Medicaid in his 20219-2021 budget proposal, and just like in 2019, the policy played a large part in Evers’ 2021-2023 budget. Evers and Democrats claimed the expansion was necessary because it would expand access to healthcare and draw down billions of dollars from the federal government.
Republicans on Joint Finance were a “no” on Medicaid expansion from day one. The expansion was removed from the budget when JFC removed over 390 proposals from Evers’ proposal. Along with the expansion, JFC removed proposals that would have given extra state subsidies to people who earn up to 250% of the federal poverty line to pay for insurance premiums, eliminated copays on prescription drugs purchased by Medicaid enrollees, capped copays on a month’s-worth of insulin to $50, and created a new commission to regulate prescription drug prices with the strong-arm of the government.
Evers’ proposed DHS budget would have spent $31.5 billion All-Funds and $9.3 billion GPR, a $715 million GPR increase and a $5.4 billion All-Funds increase over last biennium. Instead, Joint Finance passed a budget that spends $30.1 billion All-Funds and $8.86 billion GPR on DHS.

Medical Assistance And Why Medicaid Expansion Is Wrong For Wisconsin
The largest line-item in DHS’ budget each year goes to Medical Assistance, or MA. MA provides government-funded healthcare for the poor, disabled, and elderly. Medicaid exists under the MA umbrella and provides healthcare coverage for low-income individuals.
Wisconsin has already invested a great deal into our MA program, making it one of the country’s most generous. From 2009 to 2019, Wisconsin invested $92.4 billion all funds, including $25.5 billion General Purpose Revenue (GPR) funds into MA. In 2019 alone, the State of Wisconsin invested $10.66 billion all funds, $2.84 billion GPR on 1,123,000 MA recipients.
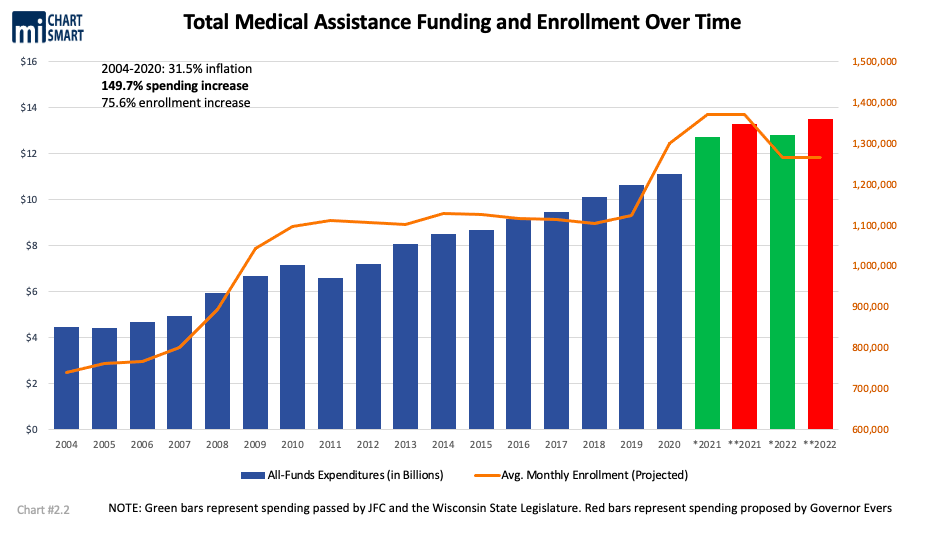
In the 2021-2023 budget, the cost to continue Medicaid at current level is $2.7 billion All-Funds and $547.7 million GPR.
Despite all that spending just to maintain our Medicaid services, Governor Evers and Democrats still wanted to spend more this budget on the program and add on tens of thousands of more enrollees. The federal government tried to bribe Wisconsin with $1.6 billion in federal incentive dollars if the state expanded eligibility to an additional 90,000 more low-income enrollees. It is unknown how many of those 90,000 individuals would even be interested in enrolling.
Democrats claimed that expansion was necessary to deliver healthcare access to poor Wisconsinites, but that ignores the effectiveness of Wisconsin’s existing system.
For one, of the 90,000 new enrollees Evers and Democrats say would benefit from expansion, half already have healthcare coverage. The other half of the 90,000 have access to affordable subsidized healthcare on the federal Obamacare exchange. Wisconsin is the only state that has not accepted expansion, but does not have a coverage gap. Everyone in our state who is not eligible for Medicaid, but is between 100-400% of the federal poverty line, has access to subsidized, affordable, private insurance.
For another, Medicaid expansion is no free lunch. Even if the federal government says they’ll take a $1.6 billion load off of Wisconsin’s Medicaid bill, Wisconsinites would still have to foot the bill for 10% of new enrollee’s coverage with their state taxes, while paying the other 90% with their federal taxes. Medicaid expansion in states like Oregon and Minnesota has also wreaked havoc on their state budgets because of unexpected increases in enrollees, leading to sudden cost hikes to the state. Expansion could bring the same harmful effects to Wisconsin
Wisconsinites up to 100% FPL have access to Medicaid, & those between 100-400% FPL have access to the subsidized federal exchange.
At 100.1% FPL, many WI people can get exchange plans for around $20 per month.
Wisconsinites already have access to affordable healthcare coverage pic.twitter.com/TPBrD97ROm
— MacIver Institute (@MacIverWisc) May 25, 2021
Finally, per analysis by the nonpartisan Wisconsin Legislative Fiscal Bureau, data shows that the more people there are enrolled in Wisconsin’s Medicaid program, the fewer providers would accept the insurance. More Medicaid equals lower healthcare access, defeating a major part of Democrats’ and Evers’ arguments for the expansion.
Evers’ Medicaid expansion proposal also included a repeal of work requirements for childless adults as a condition of staying on Medicaid. If that were removed, Evers would further incentivize certain people to stay out of the workforce and remain on the government dole. A move like that would further stress the employment shortage that Wisconsin is already dealing with this year while many working-age adults live off of federal unemployment boosters.
Republicans pushed back against every attempt to pass expansion this session. Legislators like Co-Chair Born and Senator Mary Felzkowski repeatedly asserted that they don’t don’t want to send low-income Wisconsinites onto the Government dole when they already have a private solution to healthcare access.
In the end, the Legislature passed and the Governor signed an MA budget that spends $25.6 billion All-Funds and $6.9 billion in GPR. The budget still increases Medicaid funding by over $700 million GPR compared to the last biennium, but not nearly as much as Evers’ proposed $26.8 billion All-Funds and $7.2 billion GPR spending increase.
Major Republican Investments In Public Health And Medicaid Reimbursements
While Democrats lamented another failed attempt to expand Medicaid, Republicans got to work on including new healthcare investments into their budget.
Republicans included a plan that increased MA cost reimbursements to nursing homes by $20 million per year, increased funding for direct care services by $104.2 million All-Funds, and increased MA reimbursements to boost the hourly pay of personal care workers to $20.69. These were welcome changes after the coronavirus exposed the needs and staffing gaps in nursing, assisted living, and personal care fields.
The budget also extends Medicaid postpartum care from 2 months to 3 months, increases the reimbursement rate of EMS and ambulance services to 80% with a $6.7 million GPR increase, and increases MA reimbursements to dentists by $18.5 GPR, $46.3 million All-Funds. That equals a 40% reimbursement increase for Medicaid-serving dentists. Gov. Evers had proposed $14.3 million GPR for a 23% reimbursement increase.
The budget also contains a $30 million increase to the maximum annual amount allotted for the state Obamacare reinsurance program. The maximum amount the state was allowed to use to buy down Obamacare exchange premiums until now was $200 million.
The Governor and the Legislature agreed to invest $40 million GPR more in disproportionate share hospitals (DSH) in the budget. Outpatient mental health and substance abuse services saw a 15% reimbursement increase under the budget, and child and adolescent day treatment services saw a 20% increase, for a total $9.6 million GPR, $23.9 million All-Funds boost. Evers proposed increasing reimbursements to both services by 40% with a $40.7 million All-Funds investment.
Opioid treatment providers will also see a 5% reimbursement rate increase under this budget, equalling $1.5 million GPR more. Governor Evers wanted to spend $4.35 million more GPR on the providers for a 20% reimbursement increase.
With a projected $5.87 billion surplus in state coffers by the end of the biennium, JFC chose to invest even further into MA reimbursements for other services that weren’t noted by the Governor. Speech-language pathology received a $1.15 million GPR reimbursement increase under the JFC budget, audiology received a $562,200 GPR increase, chiropractic care got $1.7 million GPR more, and physical therapy received a $892,000 GPR increase.
Joint Finance Co-Chair Born said that the budget contains more investments in healthcare than some areas of even Governor Evers’ proposed budget, all without accepting the Medicaid expansion.
Health Equity Scheme And “Public Option” Axed
The Joint Finance Committee also axed a list of non-fiscal “health equity” initiatives, which include a $25 million non-medical Medicaid community health benefit, $30 million in “health equity grants,” and a “Health in All Policies Action Team.” None of these had much to do with health at all, and had much more to do with Evers’ radical, whole-of-government race equity agenda, rooted in Communist-style orchestration of outcomes. Taxpayers can be relieved that their dollars will go towards other, less partisan initiatives than these.
Evers proposed a “public option,” to start by 2025, that JFC nixed as well. A public option is a government-run, taxpayer-funded healthcare plan made to compete with private insurers on the market. Leftist proponents of the plan say it would increase competition and lower insurance premium costs market-wide. In practice, however, the Cato Institute describes the public option as “merely a slower and more politically feasible way to achieve the destruction of private health insurance.”
On their own, public option plans don’t have a record of increasing competition or lowering any premiums, and they do not tend to offer lower premiums than those on the private market. Writing for the Heritage Foundation, Edmund F. Haislmaier and John C. Goodman say “the government would need to rig the market” in order to deliver on the promises politicians have made about the plans. This rigging would play out “not only by requiring doctors and hospitals to participate, but also by forcing them to accept lower fees than those charged to its competitors.” This makes the public option, first, a recipe for hardship for doctors and the medical industry, similar to Obamacare. Second, when the government tips the scales in order for a public option to compete, the government squashes out the private competition, thereby restricting healthcare options for the patient.
For public options to function, they would have to be the only option. We’re pleased to see this expansion of government micromanagement removed from the state budget.
Evers Makes Modest Healthcare Vetoes, With One That Saves Taxpayer Money
The Governor’s healthcare vetoes were nothing earth-shattering. Evers made some technical changes to the Legislature’s provision on expanding psychiatric beds in northern Wisconsin. His partial veto struck language that required that only specific health systems be deemed the primary receivers for emergency detentions. His veto provides more flexibility for someone in a psychiatric emergency to go to a facility for help that may be closer to their home than a facility in Eau Claire or Chippewa counties. He also made a partial veto on a provision requiring DHS to compile a list of behavioral health beds for a statewide bed tracker. He claimed this provision was “burdensome” to DHS because information on “crisis stabilization beds” and other bed operators around the state is difficult to find.
Evers made another partial veto to a provision that allocated $250,000 GPR for DHS to distribute grants to employers that organize employee blood drives. DHS would have delivered grants worth $20 per blood donation collected. The Governor deleted the part of the provision that set grant amounts at $20 per donation because he objects “to compensating employers for their employees’ blood.” We agree. Plus, it shouldn’t be the government’s place to pay employers taxpayer money to facilitate charitable medical donations.