
Dan O’Donnell systematically debunks Governor Evers’ claim that the state mysteriously added nearly 1,000 nursing home deaths to its total last week because investigators just couldn’t determine where the deceased had lived.
March 26, 2021
Perspective by Dan O’Donnell
It’s not just that Governor Evers is lying about why his Department of Health Services (DHS) undercounted COVID-19 deaths in the state’s nursing homes by nearly 1,000; it’s that he is so obviously and probably lying.
When asked this week why DHS officials quietly upped the number of nursing home deaths from 1,956 to 2,927, Evers rather perplexingly claimed that state investigators simply couldn’t figure out where thousands of COVID victims lived.
“Our local folks got lots of death certificates and death investigations that just had a street name on it,” he said. “How do we know that is a nursing home?”
This just isn’t true. If it were, then the State of Wisconsin hasn’t managed to find a home address for a staggering 37% of the people who died of COVID-19 over the past year. That’s either terrifying incompetence or, far more likely, sickening dishonesty.
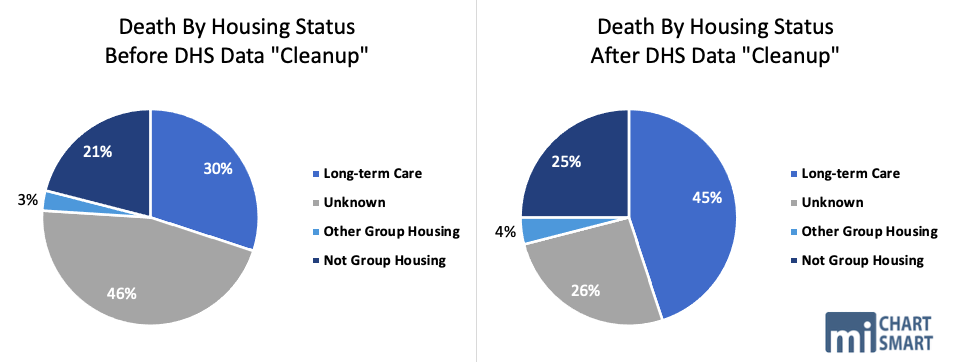
In late October, the Milwaukee County Medical Examiner’s Office created a spreadsheet of every COVID-19-related death in the county to date. Of 481 deaths, only three did not have a home address listed. How does Milwaukee County know 99.4% of its COVID victims’ addresses, but Wisconsin knows only 63%?
If the patient died in the nursing home in which he or she lived, it would obviously be easy to determine a home address, so Evers’ claim is that it was impossible for state investigators to determine where they lived since they just showed up at the hospital and then died.
This is impossible, at least to the extent Evers claims that it did.
“I’m an emergency room nurse in the largest ER in Southeastern Wisconsin,” said one source, who did not wish to be identified because her employer did not authorize her to speak on the record. “When we do death paperwork on a patient, we have to list where they came from, specifically if they came from a skilled nursing facility.
“Even in emergency situations, unless the person is found lying unresponsive outside (and even then, we are pretty damn good at finding identification and addresses) we always know where patients are coming from. We would never let an EMS crew leave the department without giving us an exact facility and location the patient came from.”
“I have never once in all my years doing admissions not known where a patient came from,” said another source, who works in hospital admissions and is also not being identified because he is not authorized to speak on the record. “If they come from a nursing home, we know it. If they come from a house, we know it. If they’re homeless, we know it.”
The location from which a patient is referred to a hospital is known in the medical field as the “point of origin,” and it is a necessary piece of demographic information for processing patients. Epic Systems software, which is used by most medical facilities in Wisconsin, won’t allow a patient case to be closed without entering a point of origin.
A “Visit Code 5” is a patient who was admitted “as a transfer from a Skilled Nursing Facility (SNF), Intermediate Care Facility (ICF), Assisted Living Facility (ALF) or Nursing Facility (NF) where he or she was a resident.”
“5” is universal shorthand for a patient who was transferred from a nursing home, and every hospital in the state would be expected to keep a record of each patient’s point of origin and home address (if the patient had one).
Even DHS’ own ForwardHealth Medicaid management program uses it, and it cannot process claims from health care providers if they don’t “enter a code indicating the source of the admission in the Point of Origin field” in their online claim forms.
“I work in medical coding,” explained another source. “It is required that every patient who comes to the emergency room or is admitted to the hospital has a point of origin. They are very specific, and Medicare/Medicaid will not accept a claim without it. Wisconsin’s own ForwardHealth states that this is required, and claims will be denied without it.”
In light of this, why did DHS Deputy Secretary Julie Willems Van Dijk claim that investigators just had no way to know victims’ home addresses?
“When case and death data were put into our disease surveillance system, it was common for some fields to be left empty or boxes to be unchecked due to the inability of the disease investigator to collect that particular information,” she explained while announcing last week that DHS nursing home death numbers had been surreptitiously changed.
This seems to be the Evers Administration’s story, and they’re sticking to it, even in the face of objective information that thoroughly debunks it. See the MacIver analysis of the data here – DHS, Once Again, Failed To Provide Accurate And Complete Data To The Wisconsin Public.
“This is not something that you should have to go back and correct after the fact,” Harvard University health care policy professor David Grabowski told The Milwaukee Journal Sentinel. “You can look at 40-some (other) states that seem to be able to do this in real-time.”
The painfully obvious reason is that determining a point of origin and home address for COVID-19 patients is remarkably easy to do—except, it would seem, for the Evers Administration.
And Wisconsinites should demand to know why. Evers’ ridiculous explanation needs to be called out for the lie that it is and recognized for what it is designed to do: Get people to stop asking questions.
That’s the thing about lies, though. They always seem to lead to more questions…and more problems.
